
Radiation Induced Lung Injury (RILI)
The development of radiation-induced lung injury (RILI) is a potentially fatal toxicity in cancer patients undergoing thoracic radiotherapy or in individuals exposed to ionizing radiation (IR) from a nuclear incident. The pathobiology of radiation pneumonitis and radiation-induced lung fibrosis (RILF) is complex but includes the deleterious effects of unchecked inflammation (reactive oxygen species, cytokines, inflammatory cells) that increase vascular permeability, impair gas transfer and promote fibrosis. Radiation-induced lung injury, including radiation pneumonitis and radiation fibrosis, is common among patients who have received radiation therapy, and it is the most common treatment-limiting toxicity among patients who receive thoracic radiation. The clinical presentation is typically cough, low-grade fever, with or without dyspnea, and radiographic changes that demonstrate a pattern of pneumonitis with ground glass opacities. It typically presents one to six months after therapy, while radiation-associated fibrosis tends to present six to twenty-four months following radiation therapy.
Early radiation effects manifest as radiation pneumonitis. Radiographic findings of lung injury are more much common than clinical symptoms of radiation-induced lung injury, and frequently occur in the area of the lung exposed to radiation. Early lung injury tends to occur one to three months following radiation treatment, but can present as late as six months after radiation exposure. The severity of lung injury varies widely among patients, ranging from asymptomatic to severe respiratory failure and death.
Late radiation-induced lung injury typically presents as pulmonary fibrosis. These findings are generally visible radiographically by six months, and almost all patients who develop radiation-induced pulmonary fibrosis show evidence by twenty-four months following radiation exposure. Although individuals with pneumonitis are more likely to develop radiation-associated fibrosis, not all patients who develop fibrosis have a history of radiation pneumonitis.
Cause
Radiation-induced lung injury is due to direct–and potentially indirect–damage of lung tissue. Radiation treatment generates reactive oxygen and nitrogen species that produce oxidative injury to cellular structures and result in cellular death. Type I pneumocytes, the primary lung cells, are injured by radiation. Type II pneumocytes, which are less common than Type I pneumocytes and can de-differentiate into Type I pneumocytes, are stimulated by radiation exposure and exhibit hyperplasia and growth following such exposure.
The initial injury is thought to be due to cell death with subsequent disease and pneumonitis as a result of damage to the alveolar/capillary membrane and subsequent interstitial and alveolar edema. The fibrotic injury is due to remodeling of the initially damaged lung tissue.
Risk Factors
The risk of developing radiation-induced lung injury was thought to be related primarily to the total dose of radiation delivered. Radiation pneumonitis rarely presents among patients treated with a dose of less than 20 Gy, while it almost always presents among patients who are treated with doses at 40 Gy or greater.
However, more recent studies suggest that the volume of the lung that receives more than 20 Gy (V20) and the total volume of lung spared from radiation exposure are better predictors of which patients will develop radiation-induced lung injury. In addition, patients who are treated with chemotherapy–especially those treated with actinomycin D, adriamycin, bleomycin, and busulfan–are at greater risk of injury, as these agents are known to potentiate the effects of radiation on the lungs. Older patients are at increased risk of radiation injury, as are patients whose neoplasms are located primarily in the lower lobes of the lung. More recent studies also suggest that pre-existing subclinical interstitial lung disease is a significant risk factor for both development of radiation pneumonitis and increased severity of disease.
Insight
Pulmonary radiation injury manifests in approximately 8 percent of patients who receive thoracic radiation. However, reports of the incidence of symptomatic radiation pneumonitis range from 1-34 percent of patients who receive thoracic radiation for malignancy. Similarly, approximately 43 percent of patients who are exposed to thoracic radiation therapy have radiographic evidence of radiation pneumonitis, although estimates range widely from 13-100 percent.
ALT-100 Benefits
Radiation-induced lung injury (RILI) is a serious lung toxicity of ionizing radiation in patients receiving radiotherapy (for a variety of cancers) with radiation-induced pneumonitis and fibrosis; both potentially lethal outcomes. Current therapies for RILI are extremely limited with only high dose corticosteroids as a controversial treatment with limited efficacy at best and with serious toxicities.
Our preclinical studies utilizing whole lung thoracic irradiation (WTLI), identified a cytozyme, nicotinamide phosphoribosyltransferase (NAMPT), as a novel RILI therapeutic target given its capacity to potently induce lung and systemic inflammation. We have also shown that NAMPT expression and secretion is markedly increased by radiation and is a key contributor to RILI development and severity.
Aqualung has generated ALT-100, the eNAMPT-neutralizing, humanized monoclonal antibody as a therapeutic agent to treat RILI by reducing the inflammatory cytokine storm which leads to organ dysfunction. It is this organ dysfunction which leads to potential morbidity and mortality.
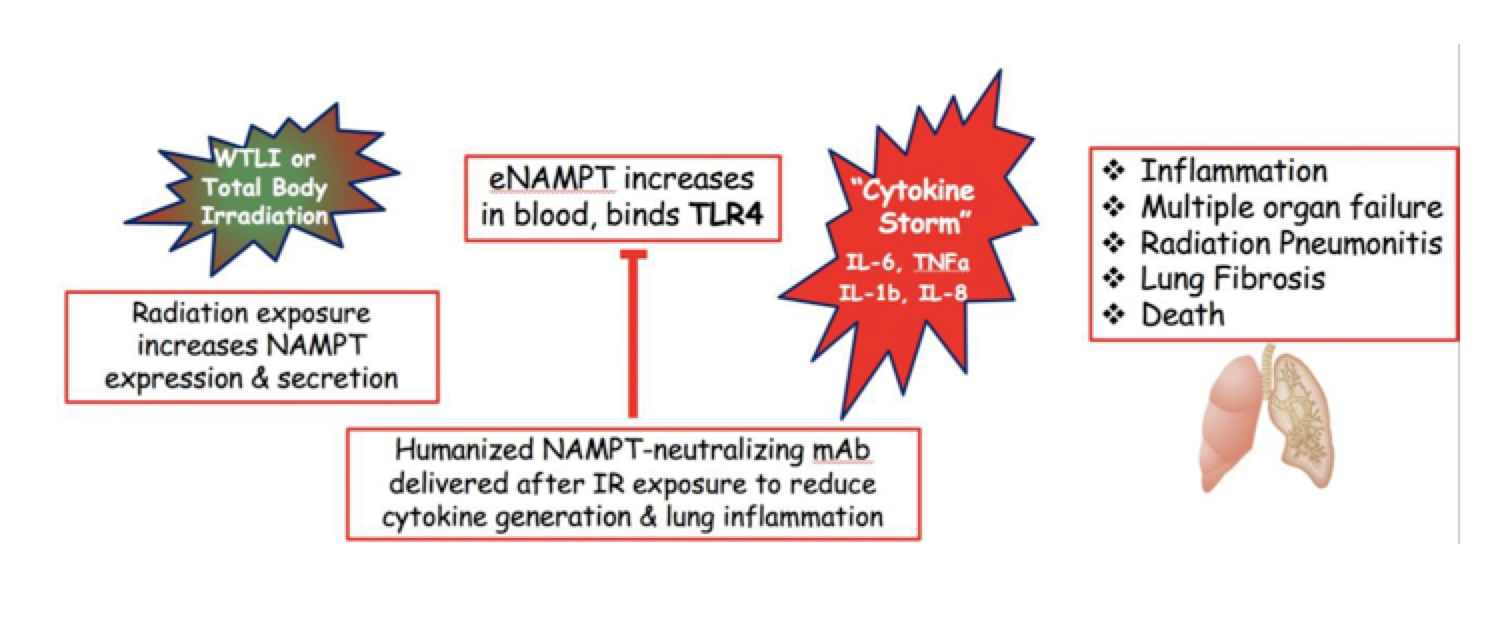
Targeting IR-induced cytokine storm and lung and systemic inflammation with the eNAMPT- neutralizing humanized mAb, ALT-100, to limit and reduce IR-induced morbidity and mortality